Overview
The knee is a hinge joint where the femur, tibia, and patella articulate through three compartments of cartilage. When that cartilage wears through across multiple compartments — the hallmark of tricompartmental osteoarthritis — standing, walking, and stairs become painful and the leg can bow or buckle.
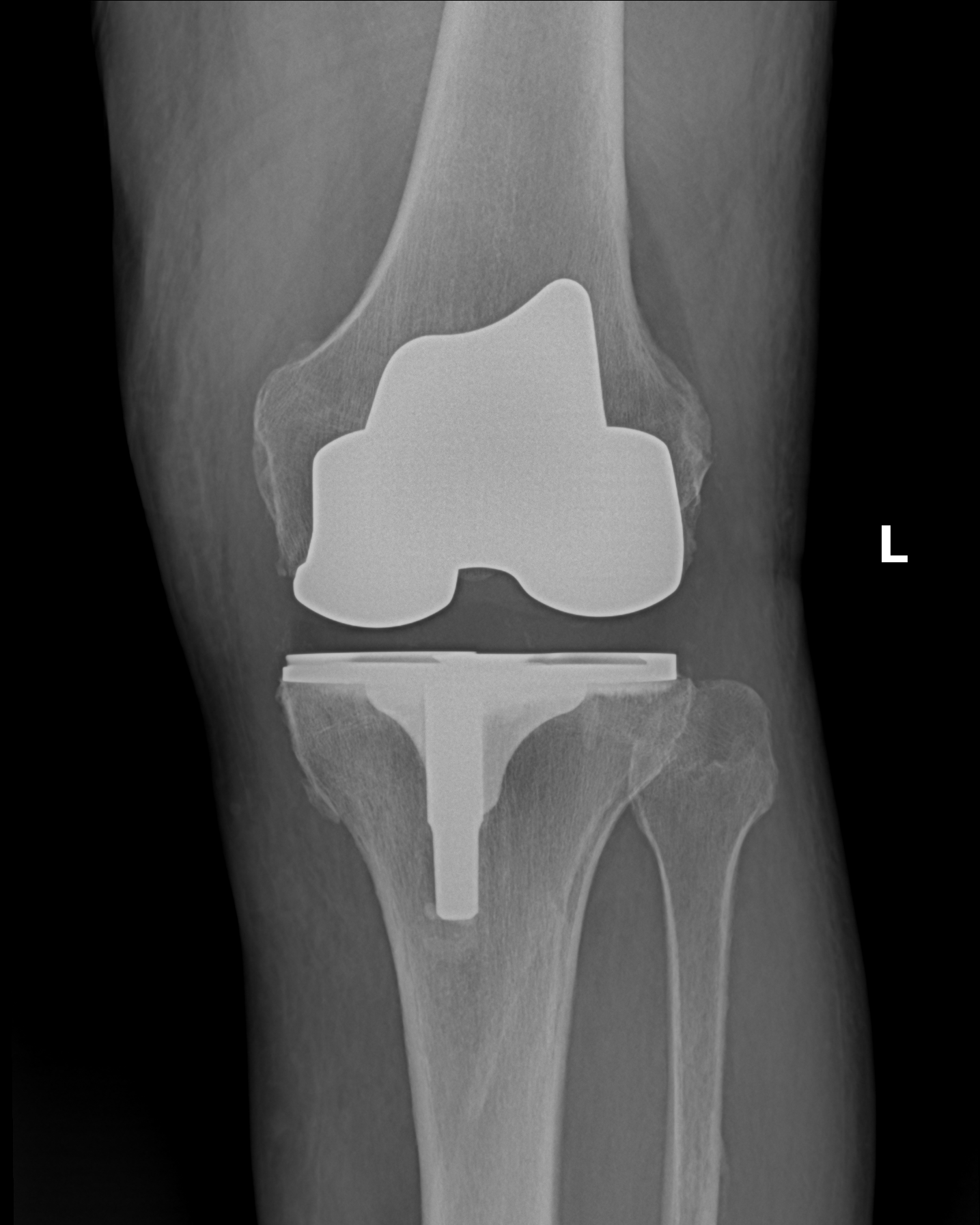
"Total knee replacement" is the standard name for this operation, but a more honest description is knee resurfacing. The knee itself is not removed. The damaged ends of the femur, tibia, and (usually) the back of the kneecap are shaved by a few millimeters and re-capped with metal and polyethylene. Most of the native bone, the ligaments on the sides of the knee, and the surrounding soft tissue are preserved. Patients sometimes arrive expecting a wholesale swap of the joint — it is a smaller operation than that word implies, and one reason recovery and long-term function are as good as they are.
How the Procedure Works
We remove the damaged cartilage and a measured layer of bone from the femur, tibia, and typically the back of the patella — no more than necessary, because bone removal is permanent. Metal components are cemented or press-fit onto the femur and tibia, with a polyethylene spacer between them. The part of the procedure that most affects the outcome isn't implant selection; it's gap balancing and alignment. We check flexion and extension gaps with trial components in place: if the knee is tighter in flexion than extension, or vice versa, we adjust the tibial cut and soft-tissue releases until both gaps match. A knee that is well-balanced and properly aligned will track smoothly, bear load evenly, and feel stable through the full arc of motion. One that is not will hurt and wear asymmetrically regardless of implant brand.

When to Consider Total Knee Replacement
Total knee replacement is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:

Advanced tricompartmental arthritis
Cartilage loss across multiple compartments on weight-bearing X-rays, with daily pain and functional loss.
Exhausted non-operative care
Failed extended course of anti-inflammatories, physical therapy, weight loss, bracing, and intra-articular injections.
Deformity or instability
Progressive varus or valgus deformity, or a knee that buckles — both signal that the joint is no longer supporting the limb.
Conditions This Treats
Physicians Who Perform Total Knee Replacement



Providers Who Surgically Assist with Total Knee Replacement


Risks & Why We Still Recommend It
Every operation carries risk. The reason we offer this procedure is that the condition, left untreated, causes daily pain at rest and with walking, progressive deformity, and a leg that can no longer reliably bear weight. That is the trade we are managing — not eliminating risk, but choosing the smaller of two unfavorable trajectories.
The risks we discuss with patients before total knee replacement include:
- bleeding and infection (including rare deep periprosthetic infection)
- anesthesia risk
- blood clot (DVT/PE) — mitigated by perioperative prophylaxis
- stiffness that sometimes requires manipulation under anesthesia
- persistent pain from component malposition or soft-tissue imbalance
- periprosthetic fracture
- polyethylene or component wear over time, eventually requiring revision
- rare nerve or vessel injury around the popliteal space
If you have had a prior knee replacement
If you have a knee replacement — from here or from elsewhere — and are experiencing new pain, instability, swelling, or stiffness that is not settling, call our office before booking a clinic visit. Dr. Vrana takes care of knee-replacement revision here when the case fits the practice; some revisions are better handled at a revision-specialty center, and our team can usually tell on the phone which your case is. We would rather save you the trip than see you for something we would have to refer out.
The indication to proceed is end-stage tricompartmental arthritis with daily pain and functional loss that has not responded to a full course of non-operative care. Patients who don't need this operation don't get it.
Further Reading
External patient-education references and related OSI pages for additional background: