Overview
When the rotator cuff is irreparable, an anatomic shoulder replacement will not work — the ball will not stay centered in the socket without the cuff. The reverse design solves that biomechanical problem by swapping the articulation: the ball is fixed to the glenoid and the socket to the humerus. This moves the center of rotation medially and downward, giving the deltoid the leverage to lift the arm even when the cuff cannot.
How the Procedure Works
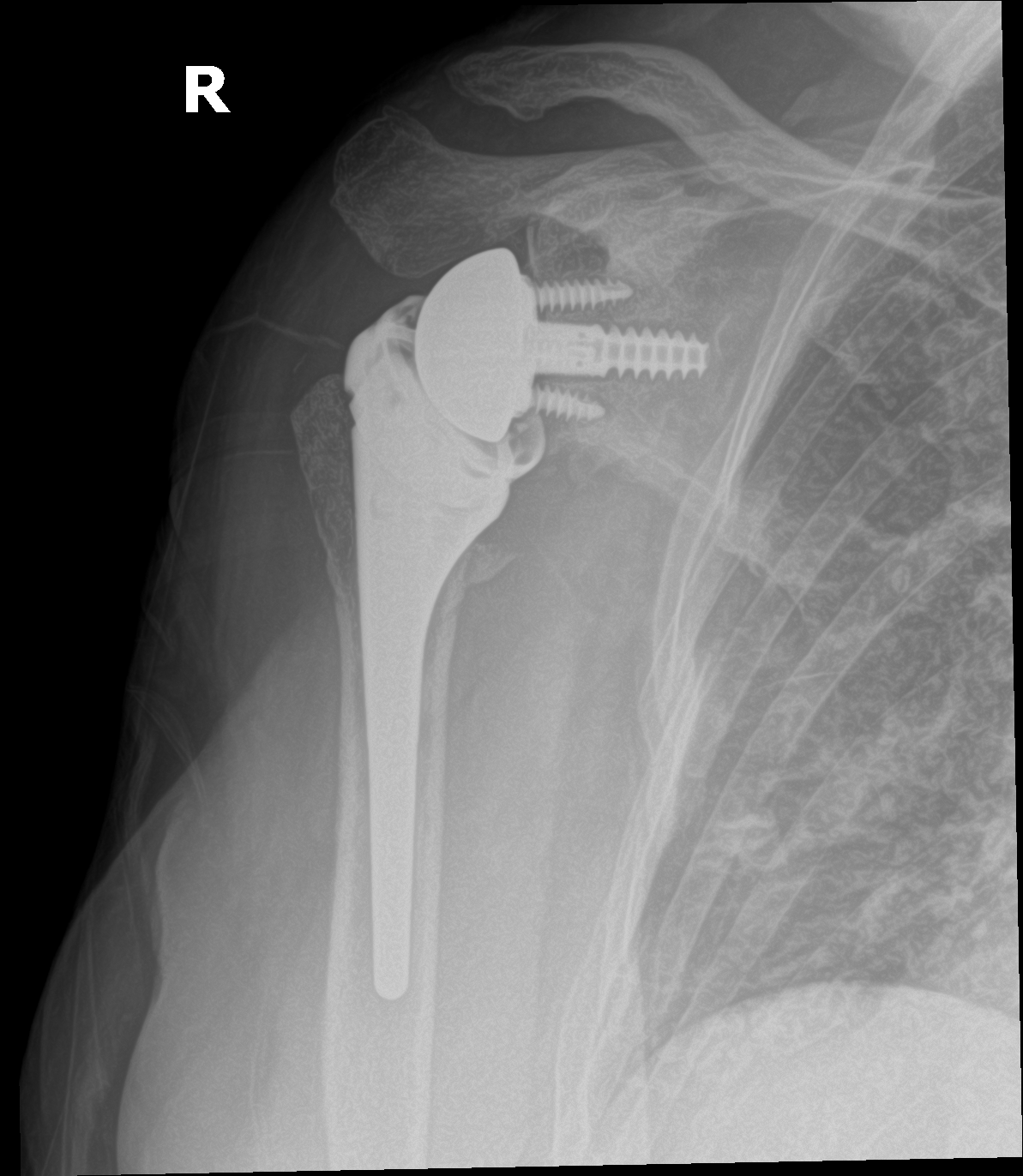
The critical step on the glenoid side is baseplate fixation: the central peg or screw must engage the strongest bone at the glenoid vault, and peripheral screws are directed to maximize pull-out strength — a loose baseplate is the most consequential failure mode in this operation. The glenosphere is then locked onto the baseplate. On the humeral side, we choose stem length and offset, then set the polyethylene socket height to tension the deltoid: too little tension and the joint dislocates, too much and the patient loses comfortable motion and risks scapular notching. We check range of motion and stability with trial components before committing to final implants. The remaining deltoid does all the work from this point forward — the implant geometry provides the lever arm the cuff can no longer provide.
When to Consider Reverse Shoulder Replacement
Reverse shoulder replacement is generally offered when symptoms, imaging, and a trial of non-operative care together point to surgery as the next step. The typical picture includes:
Rotator cuff arthropathy
Long-standing rotator cuff deficiency leading to cuff tear arthropathy — arthritis in a cuff-deficient shoulder.
Massive irreparable cuff tear
A huge cuff tear with pseudoparalysis — the inability to actively elevate the arm.
Failed prior shoulder replacement
Revision from a failed anatomic replacement or fracture hemiarthroplasty.
Conditions This Treats
Physicians Who Perform Reverse Shoulder Replacement



Providers Who Surgically Assist with Reverse Shoulder Replacement


Risks & Why We Still Recommend It
Every operation carries risk. The reason we offer this procedure is that the condition, left untreated, causes a shoulder that cannot actively elevate the arm — the combination of arthritis and an irreparable cuff leaves patients unable to reach a shelf or comb their hair. That is the trade we are managing — not eliminating risk, but choosing the smaller of two unfavorable trajectories.
The risks we discuss with patients before reverse shoulder replacement include:
- bleeding and infection (including rare deep periprosthetic infection)
- anesthesia risk
- dislocation of the reverse construct
- acromial or scapular-spine stress fracture
- component loosening over the long term
- scapular notching
- nerve irritation (axillary, transient)
- blood clot (rare in upper-extremity surgery)
The indication to proceed is cuff-tear arthropathy, massive irreparable cuff tear with pseudoparalysis, or complex proximal humerus fractures in older patients. Patients who don't need this operation don't get it.
Further Reading
External patient-education references and related OSI pages for additional background: